

It’s one of the most intractable areas of focus in all of vascular disease, and the source of—inarguably, Brajesh K. Lal, MBBS, emphasizes—the most intensely studied vascular surgical procedure anywhere in the sphere of the specialty. And for some years, Lal has had the development of a more accurate method of risk assessment for this perennial vascular problem fixed firmly in his sights: carotid disease.
Now, the Baltimore-based director of the University of Maryland’s Center for Vascular Diagnostics and the National Institutes of Health Vascular Imaging Core Facility may be a little closer to his target.
Lal is speaking to Vascular Connections shortly after he delivered the interim findings of the CRISP trial during Scientific Session 9 at SVS ONLINE on July 2. Lal and colleagues had unveiled data on the novel application of artificial intelligence (AI) algorithms to more successfully risk stratify those with carotid atherosclerosis. They demonstrated,
he told the digital conference, that a composite of carotid plaque geometry and tissue composition, patient demographics, and clinical information “has a better predictive performance for major adverse neurological events [like stroke] than the traditionally utilized degree of stenosis alone.”
The company behind the AI, Boston-based Elucid Bio, proudly announced ahead of Lal’s SVS ONLINE presentation that the technology in question, called vascuCAP, had shown a more than 70% improvement in accuracy of stroke prediction as compared to stenosis-based guidelines over a six-year time period.
But in order to get to the heart of Lal’s current risk prediction quest, he first takes Vascular Connections on a little history tour of carotid disease.
Those studies to which he draws reference—beginning in the 1970s and continuing unabated through today— were united in their search for the best treatment for asymptomatic carotid stenosis patients.
And all of them indicate that “if you take 100 people with asymptomatic carotid stenosis and perform carotid endarterectomy [CEA], and randomize 100 people with asymptomatic carotid disease and give them the best available medical therapy,” the patients who received a CEA did a little better,
Lal says. Yet, the challenge remains that, even among those who did not undergo surgery, stroke rates were “not tremendously high.” If those 100 patients are followed, about two per year suffer a stroke.
“What the clinical standard of care is—that if you select patients based on the degree of stenosis—and the only clinical risk stratification tool across the world is percentage stenosis, selecting patients based on this only lets you identify a subgroup of patients where 2% of them are going to develop a stroke. When you think about it, it’s not a very sensitive or specific risk stratification tool. It’s the best we have.”
The bottom line: Percentage stenosis is not the ideal way to risk stratify patients in order to identify those who will have a stroke. The research group worked across four centers, and recently added a fifth.
“We were able to collect a reasonably large cohort of patients,” Lal says. “It’s a very unique cohort—asymptomatic carotid stenosis at baseline—and at least two CAT scans performed at least two months apart. So we could also study how the plaque was changing over time.”
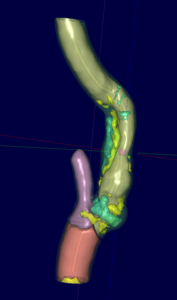
Armed with all of the demographic and clinical features of the cohort, as well as the geometric features of the plaque, including percentage stenosis, Lal and colleagues got to work on neuro-network analysis—where the vascuCAP AI component steps into the fray.
“We essentially poured all of thjs data into a series of multiple progression models, neuro-network models, all sorts of multivariable, analytic models, and all sorts of combinations,” he says. “The algorithm then selects out the one that provides the best model, so there’s a very objective way in which the neuro-network does this. And the best model has the best combination of sensitivity and specificity using the best combination of features.”
What this amounted to, Lal goes on, was new ground being broken: “For the first time, we were able to quantify what the sensitivity and specificity of the percent stenosis predicting a stroke is.” In short, he says, this “utilizes morphologic characteristics of the plaque. When you do that, you get a fairly good sensitivity and specificity in terms of predicting a risk for stroke.”
That’s where the research program stands at this point: modality identified, confirmation it can be performed in a standardized fashion, identification of means of image analysis, correlating this with histology, and, finally, finding software to accelerate post- processing. In terms of the final piece in this timeline, muses Lal, that means bringing processing down “from three hours to about 15 minutes.” So where do the researchers go from here?
“The next step is to use a retrospective dataset to demonstrate proof of concept,” Lal says. “And the final step is going to be to identify a prospective group of patients who are followed longitudinally. I’m talking to a bunch of people to put that together. My anticipation is—looking at these numbers—we’re going to need about a 600-patient study. This has already become a 200-person study in its retrospective analysis, and I don’t think it will be a problem identifying 600 people.”
Lal is loath to describe these developments as a disruptive innovation. But he believes that if the current trajectory of his team’s research is maintained, this could be a game changer in asymptomatic carotid disease risk stratification. “I look at it this way,” he says: “The European Society for Vascular Surgery guidelines have very emphatically introduced the concept that we have to move beyond degree of stenosis. Everybody has intuitively known that, but for the first time we are beginning to talk about it in our guidelines.
“The Society for Vascular Surgery guidelines, which are in the making as we speak, are most likely going to be incorporating statements regarding that, too. We all as clinicians know we have to move beyond percent stenosis. It’s not effective, it’s not sensitive and it’s not specific. So what I can say, without using any adjective, is that if this story continues the way it is—and I have no reason to believe that it won’t because we’ve been very rigorous in how we’ve analyzed our data—I think this has the potential to the change way we risk stratify patients, and select patients for interventions in those who have asymptomatic carotid disease. It’s a very exciting and very interesting development.”
In a nutshell, results so far have assured Lal of something important: “For the first time, plaque assessments have become reliable with a reachable technology. They were always reliable if you were willing to spend $2,500 per scan, another three hours of post-processing time, which is also money, and surface coil, which is $30–40,000 on top of a million-dollar MR machine. Before you know it, you’ve essentially priced yourself out of a clinically applicable tool. Now plaque imaging is coming within clinical reach. I truly believe it’s just a matter of time.”











