
It all started with a “we should do research together; this is fascinating.” The result—the production of a prototype eyewear that decreases radiation to the eye and brain—is the more-than-decade-long toil of Melissa Kirkwood, MD, and colleagues at UT Southwestern in Dallas, Texas. From conference podium to conference podium, through endless research studies and paper-writing, Kirkwood has put in the miles to get the disposable, lightweight shield patented. Here, the UT Southwestern vascular chief tells Vascular Specialist about her journey and production of the “much-needed” device aimed at helping surgeons and interventionalists combat radiation exposure.
VS: Can you give an overview of your research journey in radiation so far?
MK: Yes, about 11 years ago our vascular division was flagged for having a high radiation dose case. The case involved a physician-modified aortic stent graft in a morbidly obese patient. Because of this, our radiation physicists had to come and speak with us as a group. I was fascinated by the topic and what they were discussing. There are so many simple things that we can do to decrease our radiation dose. After this talk with the physicists, I went up to Dr. Gary Arbique and Dr. Jeffrey Guild and said, “We should do research together; this is fascinating.”
Our first project was simply looking at the radiation dose from our complex cases before and after our talk with the physicists, where we learned some tricks to decrease dose. After controlling for multiple factors, we were able to show that by implementing simple things, you can significantly drop the radiation dose. We then looked at the risk of deterministic effects, namely skin injuries in patients following high radiation dose cases. We studied this initially retrospectively and then started a prospective study, following these patients with skin exams. What we found was skin injuries are extremely rare and are likely multifactorial, with some patient predisposing factors and not solely based on dose.
Then we progressed and looked deeper, specifically at surgeon dose. We found that factors like where the surgeon stands around the table, whether the table mounted lead skirt is utilized, and what type of case is performed matters significantly. This paper showed that fenestrated aortic endovascular repairs (FEVARs) are by far the highest dose case that we perform as vascular surgeons. So then we took a deeper dive, looking only at FEVARs. We showed that not all FEVARs are equal in dose, that custom-made devices require more dose then pre-manufactured devices, and that the number of vessel fenestrations is a driver of increased dose. After this study, we focused on additional adjuncts to lower the dose during FEVARs, like using dual fluoroscopy with live digital zoom instead of magnification modes, employing a two-dimensional vessel navigator roadmap instead of an on-table 3D CT, as well as ensuring all equipment is up to date on new dose-lowering software.
Most recently, we have been focusing on what does not work for radiation. We have shown that the no-brainer surgical caps and regular leaded caps do not decrease brain radiation at all, because the radiation that hits the head is from scatter radiation already attenuated through the patient and not hitting the head at 90-degree angles. After discovering this, we questioned the effectiveness of leaded eyewear. Sure enough, we proved that leaded eyewear does not decrease eye dose at all due to the significant air gap between the face and the leaded lens. The leaded lens can only attenuate direct X-rays to the eyes, and since all the scatter is from the patient hitting the interventionalist at angles not covered by the glasses, they are completely ineffective. However, this seemed like a solvable problem. Our first attempt at this was studying the efficacy of adding leaded shielding to the lateral and inferior aspect of the glasses. This was a success. Closing the air gap between the operator’s face and their eyes significantly decreased eye dose. Yet, this design was heavy, uncomfortable and caused fogging. Therefore, we have been working on perfecting the design and have created a prototype, which is patented at UT Southwestern Medical Center. The eyewear attachment has been proven to decrease both eye and brain dose to the operator and works equally well added to leaded or non-leaded routine prescription eyewear. This was recently presented [at the 2021 Western Vascular Society meeting].
VS: What more can you tell us about the latest study?
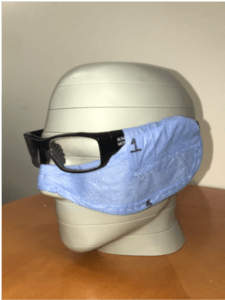
MK:. In this study, we have shown that when this prototype is added to leaded or non-leaded glasses, the dose to the lens, temporal lobe and midbrain is reduced by 85%, 81% and 71%, respectively. This means that interventionalists do not have to buy and wear leaded lenses anymore. Our prototype is just as effective when added to plastic safety glasses or prescription eyewear. The device is lightweight, detachable and reversible, so it can be used for either the right or left eye/face. Only the eye that is closest to the X-ray source needs coverage. The prototype has a sleeve for the temples of the eyewear, and then the shield is molded around the operator’s face and the inferior aspect of the lenses by a conformable wire. The adhesive strip attaches to the surgical mask, eliminating any air gap between the lower face and the eyewear. It is made of lead-equivalent shielding—sewn into soft cloth material. Even though it is disposable, it is not necessarily single use. I have worn it in multiple procedures without any decrease in efficacy. And the best part is that it is comfortable and there is no fogging. We are really excited about this shield because it is an easy adjunct that can be incorporated into daily practice to improve operator safety. When the interventionalist goes to grab his/her hat, mask, shoe covers, etc., that is the time to grab the eye/face shield too!
VS: Do you think the findings will change future practice?
MK: I hope so. Many reports have shown an increased prevalence of radiation-induced lens damage (cataracts) and brain cancer in interventionalists. The International Commission on Radiological Protection (ICRP) has set the occupational dose limit to the lens of the eye at 20mSv/year on average over five years, with no annual dose in a single year exceeding 50mSv. Thus, the results from this study have shown that with the addition of our prototype, operators can safely perform exponentially more cases and still stay under the aforementioned ocular dose threshold. We strongly believe that our design can help mitigate some of the long-term health complications that interventionalists can experience and hope that using our eye/face shield becomes standard practice to improve safety.
VS: Have there been any other recent developments?
MK: Not on this study, but we did just present at the 2022 Southern Association for Vascular Surgery (SAVS) meeting the efficacy of lower-leg leaded garments in decreasing lower body radiation dose during FEVARs. We also presented some new data on the CLEAR-MAX imaging technology system and how it lowers radiation dose on Siemens systems.
VS: What comes next for the prototype?
MK: Next steps are working with UT Southwestern to find a commercialization partner to bring the product to market. Stay tuned!











