
“Unfortunately, we are doing worse for our patients today,” were the sobering thoughts of Eric Secemsky (Boston, United States) during a late-breaking presentation in this morning’s Peripheral Arterial Controversies programme. Among several presentations on paclitaxel safety, he reported that: yes, the meta-analysis and regulatory body restrictions on paclitaxel-coated devices did cause harm through the relegation of patients to the “less durable” conventional device treatment, increasing the incidence of adverse events post-revascularisation.
In a session focused on reaching resolution on the paclitaxel controversy, early presentations given by Thomas Zeller (Bad Krozingen, Germany) and Peter Schneider (San Francisco, United States)—concerning paclitaxel-coated balloon safety in femoropopliteal occlusive disease and paclitaxel mortality across randomised controlled trials—established the “lack” of paclitaxel-coated device mortality risk in the most recent available data.
Secemsky, who presented next, gave a brief timeline of the rise and fall of paclitaxel-coated devices showing their sharp decline in use following the Konstantinos Katsanos (Patras, Greece) et al meta-analysis which reported an increased mortality risk, and the subsequent regulatory restrictions. Previously, paclitaxel devices—driven by drug-coated balloons (DCB)—were the preferred treatment for femoropopliteal intervention for peripheral arterial disease (PAD) in the United States.
Using both Medicare data and the IQVIA: Medical Device Supply Audit database, Secemsky and colleagues looked at paclitaxel device use in US hospitals between Q3 2013 and Q3 2023. He reported that, following the pivotal Katsanos et al meta-analysis, DCB and drug-eluting stent (DES) use did not recover to pre-meta-analysis levels until Q3 2023—a period of four and a half years—showing the close “parallel” trajectory between device use and emerging data, Secemsky said. The speaker also highlighted the “shrunken” downward trend in the overall femoropopliteal procedural counts in the US following the controversy, despite PAD-related amputations remaining “stable” in the same period.
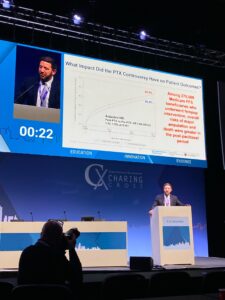
Then, Secemsky and colleagues followed 275,009 Medicare beneficiaries who underwent femoropopliteal intervention, comparing the risk of major amputation and death in the period prior to and following the paclitaxel controversy. Risk of amputation or death was reported in 40.4% and 43.2% of patients in the pre- and post-paclitaxel period, respectively. Secemsky also reported a 43.9% risk of major amputation and death in the post-COVID-19 period, establishing that risks following femoropopliteal intervention were “not driven by COVID-19 alone”, he said.
“Global restrictions on paclitaxel device use relegated thousands of patients to conventional device treatment,” said Secemsky. “The use of a less durable treatment increases the possibility of more frequent repeat interventions, the associated risks of re-intervention and the economic burden of performing these procedures.”
Although the meta-analysis and regulatory body restrictions on paclitaxel devices caused harm, Secemsky—flipping the coin—stated that it “also did good” by reiterating the need for better clinical trial practices and complete study participant follow up.
“The paclitaxel controversy not only instigated interest in non-paclitaxel therapies such as sirolimus-based treatments, but it also demonstrated that the vascular community could quickly band together to address a dispute, and particularly displayed the collaborative nature of US Food and Drug Administration (FDA) who ensured regulatory concerns were addressed,” Secemsky finalised. “These lessons can help guide the vascular community through the next controversy and to further develop evidence to shape clinical practice.”
The discussion was then opened to the FDA and UK Medicines and Healthcare products Regulatory Agency (MHRA) to provide a conclusive perspective on the matter. Representing the FDA, Ariel Ash-Shakoor (Washington, United States) began by tracing the course of the regulatory bodies’ communication to present day. Ash-Shakoor stated that, based on the “totality of available evidence” the FDA has determined that the data do not support an excess mortality risk for paclitaxel-coated devices. However, current FDA guidance when using paclitaxel-coated devices includes, but is not limited to, routine monitoring and optimal medical therapy.
Ash-Shakoor noted that lessons can be learned from the paclitaxel mortality controversy, including the importance of long-term follow up, pre-specified plans concerning missing data, and proactive patient monitoring to ensure “complete” reporting.
Providing the perspective of the MHRA, Alexander McLaren (London, United Kingdom) confirmed that no increased risk in mortality with paclitaxel-coated devices has been observed in their review of available randomised controlled trial data.
“Looking back with a critical eye to our own management of the long-running complex topic, I do feel the MHRA response was swift and decisive with the establishment and advice that we received by the expert advisory group,” McLaren stated. In his view, as “quality, robust data were slow to emerge”, delays in decision-making were inevitable. However, taking what has been learnt forward, McLaren said that the MHRA intends on improving pre-market clinical investigation and ensuring studies are “sufficiently powered and supported” to collect real-world follow-up data.











