
A major overhaul of current procedural terminology (CPT) coding for lower extremity revascularization (LER) took effect in January, introducing new codes and allowing physicians to receive dedicated work relative value unit (wRVU) credit for the use of intravascular lithotripsy (IVL) in iliac and femoral-popliteal arteries.
Luke Perry, DO, an assistant professor of surgery at Penn State College of Medicine, said the new framework represents one of the biggest shifts in peripheral procedure coding in years. “2026 is a massive year,” he said. “Essentially, the Relative Value Scale Update Committee and the American Medical Association rewrote all the codes for lower extremity billing. All the old codes, which were arranged from 37220 to 37235, got deleted.”
The updated coding structure introduces 46 new CPT codes designed to better capture the full spectrum of LER. The new codes allow physicians to treat from the iliac arteries down to the inframalleolar and also introduce distinctions between straightforward and complex lesions. Complex lesions are reserved for those that are 100% occluded.
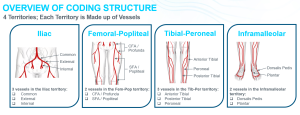
Figure 1: The updated coding structure for 2026 added the inframalleolar territory and split the femoral-popliteal territory into two vessels.
Perry said the change is intended to better reflect the technical difficulty of procedures, particularly when physicians are treating occlusions or heavily calcified disease. “If you’re dealing with an occluded vessel and you treat that, that would bill for a higher amount because it’s a complex lesion,” said Perry. “Versus just a straightforward lesion you’re angling through.”
How wRVUs factor into physician reimbursement
The coding overhaul impacts wRVUs, a productivity metric used to quantify physician work and determine reimbursement. “wRVUs are the units of measurement of productivity of a physician,” said Perry. “Essentially, they are a way the hospital systems can quantify what you do.”
Every patient encounter, procedure or intervention performed by a physician is associated with a CPT code and each CPT code carries a defined number of wRVUs representing the effort, skill and time required to perform that service. “Each one of those CPT codes has wRVUs listed to it,” said Perry. “It’s basically a measure of productivity.”
Although many physicians associate wRVUs with productivity-based compensation, Perry said the metric plays a critical role across most practice environments, including academic institutions, private hospitals and community systems. In private and community-based models, physicians are often required to meet annual productivity thresholds tied to wRVUs in order to maintain salary levels or qualify for performance bonuses.
However, wRVUs influence more than just physician pay. Perry said health systems also rely on productivity data to determine staffing needs, infrastructure investments and resource allocation. “It’s a way for hospitals to know if you need more physicians or if you can afford more physicians from a budgeting standpoint,” he said. “If you’re busy enough, can you support more vascular lab techs? Can you open up more rooms? The operating room time that you’re being given, are you utilizing it efficiently?”
Dedicated codes arrive for IVL
Among the additions to the new coding structure are dedicated add-on codes for IVL in the iliac and femoral-popliteal vessel beds. IVL, which uses ultrasonic acoustic pressure waves to fracture calcified lesions, has become a common method of vessel preparation during peripheral interventions. However, physicians performing the procedure were previously unable to bill for it separately.
“Prior to 2026, when you would use Shockwave IVL, there was no physician billing for it.,” said Perry. “Now we can bill for using IVL in the iliac and femoral-popliteal regions. It’s designated as an add-on code and you can bill up to three times, once for each vessel treated in the iliacs and up to two times, once for each vessel treated in the fem-pop. For example, if I was to do IVL on a lesion in the common iliac and a separate lesion in the external iliac, I could bill the IVL add-on code twice – once for each vessel treated. Similarly, with the femoral-popliteal region as well.”
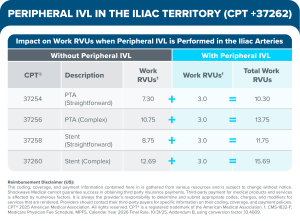
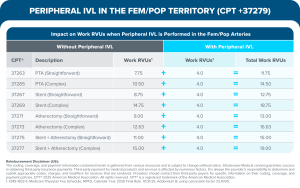
Because IVL is designated as an add-on code, it is not subject to multiprocedural reductions. Using IVL in the vessels of the iliac provides 3 wRVUs, while using IVL in the fem-pop vessels results in an additional 4 wRVUs.
How the new codes play out in practice
Perry illustrated how the new codes might apply in practice using a recent case involving a patient who presented with concern for chronic limb threatening ischemia and underwent multilevel endovascular treatment. Imaging showed near occlusion of the right external iliac, common femoral and superficial femoral arteries. He proceeded with IVL treatment across multiple segments along with stenting and drug-coated balloon angioplasty, restoring pedal pulse at the end of the case. “This case under the new 2026 codes would be considered straightforward due to not being a total occlusion,” said Perry. “And, with the new IVL codes, codes for IVL on the external iliac, common femoral/profunda and SFA/popliteal artery regions were able to be used in addition to codes for the stenting of the external iliac artery and balloon angioplasty on the CFA/ profunda and SFA/popliteal regions.”
In another example, Perry described a patient who had acute rest pain and a completely occluded iliac artery following an external iliac to below-knee bypass. “We performed IVL on the iliac and then we lined it with a stent,” said Perry. “From a new 2026 coding standpoint, this would be a complex iliac artery lesion that was treated. I would be able to bill for the stent and the add-on code of the common iliac artery IVL.” Perry noted the “complex” designation acknowledges the additional work required to cross and treat a completely occluded vessel. “Prior to 2026, there was no designation of straightforward versus complex,” he said. “Despite the fact that you treated a complete occlusion, there was not a coding and billing difference.”
Despite the expanded coding structure, Perry said some limitations remain. Dedicated IVL CPT codes currently exist only for the iliac and femoral-popliteal segments, meaning physicians performing IVL in tibial vessels still need to rely on other coding strategies.
For physicians adapting to the new coding structure, Perry said careful documentation will be essential to ensure appropriate reimbursement. “For billing and coding with the new LER coding structure, specificity in your documentation is very important,” he said. “You have to be very specific about where the tips of the wires and catheters are reporting to the most distal region. Same thing with Shockwave Javelin and balloon-based IVL, because they’re add-on codes and it’s per vessel. If you just say Shockwave of the iliac arteries, well, what segment of the iliac arteries? If you’re doing Shockwave of the common iliac, make sure very specifically you say that.”
Shockwave M5, Shockwave M5+, Shockwave S4, Shockwave L6 and Shockwave E8 Safety Information
In the United States: Rx only.
Indications for Use— The Shockwave Medical Intravascular Lithotripsy (IVL) System is intended for lithotripsy-enhanced balloon dilatation of lesions, including calcified lesions, in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, and infra-popliteal arteries. Not for use in the coronary, carotid or cerebral vasculature. Peripheral IVL is also indicated for use in renal arteries in certain jurisdictions, including the United States. Please reference Instructions For Use for country specific information.
Contraindications— Do not use if unable to pass 0.014″ (M5, M5+, S4, E8) or 0.018″ (L6) guidewire across the lesion-Not intended for treatment of in-stent restenosis or in coronary, carotid, or cerebrovascular arteries.
Warnings— Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device— Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions— use only the recommended balloon inflation medium—Appropriate anticoagulant therapy should be administered by the physician— Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Adverse effects— Possible adverse effects consistent with standard angioplasty include-Access site complications -Allergy to contrast or blood thinner- Arterial bypass surgery—Bleeding complications—Death— Fracture of guidewire or device—Hypertension/Hypotension— Infection/sepsis—Placement of a stent—renal failure— Shock/pulmonary edema—target vessel stenosis or occlusion— Vascular complications. Risks unique to the device and its use— Allergy to catheter material(s)— Device malfunction or failure— Excess heat at target site.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events. www.shockwavemedical.com/IFU
Shockwave Javelin Peripheral IVL Catheter Safety Information
In the United States: Rx only.
Indications for Use— The Shockwave Medical IVL System with the Javelin Peripheral IVL Catheter is intended for lithotripsy- enabled modification and crossing of calcified lesions in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, and infra-popliteal arteries, prior to final treatment.
Not for use in coronary, carotid, or cerebral vasculature. Additionally, not for use in pulmonary vasculature in the U.S. and New Zealand.
Contraindications— Do not use if unable to pass 0.014″ (0.36 mm) guidewire across the treatment site-Not intended for treatment of in-stent restenosis or in coronary, carotid, cerebral or pulmonary arteries.
Warnings— Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device— Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions— Avoid applying acoustic pressure pulses while IVL window is not filled with sterile saline—Appropriate anticoagulant therapy should be administered by the physician— Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Adverse effects— Possible adverse effects consistent with standard angioplasty include-Access site complications -Allergy to contrast or blood thinner- Arterial bypass surgery—Bleeding complications—Death— Fracture of guidewire or device—Hypertension/Hypotension— Infection/sepsis—Placement of a stent—renal failure— Shock/pulmonary edema—target vessel stenosis or occlusion— Vascular complications. Risks unique to the device and its use— Allergy to catheter material(s)— Device malfunction or failure.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events. www.shockwavemedical.com/IFU
© Shockwave Medical, Inc. All Rights Reserved. SPL-80263 Rev. B









