
Charles Bailey, MD, George Adams, MD and Vanessa Adams, BS, share their experience with Shockwave Javelin, the first-of-its-kind forward intravascular lithotripsy (IVL) technology that is enabling further interventional treatment for patients suffering from chronic limb-threatening ischemia (CLTI).
Peripheral artery disease (PAD) affects millions worldwide and is associated with reduced blood flow to the legs, impaired quality of life and increased risk of cardiovascular events. CLTI is the most advanced stage of PAD and carries substantial rates of amputation and mortality. Managing heavily calcified or severely narrowed lesions remains a persistent clinical challenge, particularly when device delivery is limited.
The Shockwave Javelin Peripheral IVL catheter is designed on a novel Forward IVL Platform to modify calcium in these complex lesions, enabling treatment in vessels where conventional devices may be difficult to advance and supporting a broader range of endovascular interventions.
Case report 1
Patient presentation
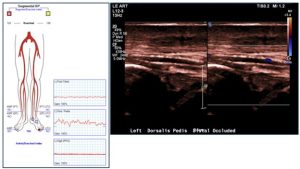
A 67-year-old man returned to the vascular clinic with left foot nocturnal rest pain and recurrence of a superficial ulceration to the tip of the fourth toe. Medical history was notable for diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure with reduced ejection fraction (LVEF 40-45%) and prior tobacco abuse. Surgical history included a prior left leg femoral-to-proximal anterior tibial artery (AT) prosthetic bypass graft (August 2025). In-office vascular lab testing revealed absence of great toe pressure and interval occlusion of the distal AT and dorsal pedal (DP) arteries (Fig 1). His bypass graft remained patent, though with diminished peak-systolic velocities throughout. Given the clinical findings of CLTI (CLTI-ischemic rest pain, recurrent digital ulceration) and a threatened surgical bypass graft at risk of thrombosis with diminished in-graft velocities and distal outflow tract occlusion, the patient was consented for a left lower extremity angiogram with possible endovascular intervention. The goal of revascularization included improved forefoot perfusion for CLTI, and to improve the outflow tract to support bypass graft long-term assisted patency.
Procedural details
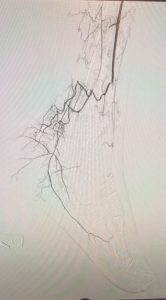
With pre-procedural imaging evidence of distal AT and infra-malleolar occlusions, an antegrade ultrasound-guided ipsilateral left femoral percutaneous access was performed. Diagnostic angiogram confirmed patency of the femoral-to-proximal AT prosthetic bypass graft, without anastomotic or in-graft stenoses. The AT was patent along its proximal and mid segments, with an occlusion noted above the malleolus and extending into the DP artery and pedal-plantar loop. Bypass graft patency was maintained via a distal branch with collateral flow perfusion to the level of the posterior tibial artery (PT) bifurcation into medial (MPA) and lateral plantar (LPA) branches (Fig 2).
A 5-Fr. by 55-cm sheath was advanced. Systemic heparinization was administered and activated clotting times monitored (ACT>250 seconds). The distal AT and DP lesions were traversed intraluminal using an 0.014 Hydrophilic guidewire with a 3.5g tip load and supportive 2.3-Fr. by 90-cm crossing catheter. The wire and catheter combination were advanced across the pedal-plantar loop and positioned in the proximal plantar artery branches, with wire exchanged for a 0.014 hydrophobic guidewire with a soft 0.7g-0.8g tip load to support device delivery. In consideration of small caliber vessels and medial calcifications throughout occluded segments, the decision was made to perform plaque and vessel wall modification with the Shockwave Javelin Peripheral IVL catheter.

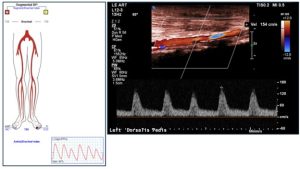
From experience, the competitive advantage of Javelin over traditional plain angioplasty balloons in this type of anatomy includes its low crossing profile and ability to safely modify plaque beyond the tip, 9, 10 creating a small lumen (1.5mm) similar to native vessel reference diameters and enabling further treatment. All the available 120 pulses were administered across the occlusive segment, with an even distribution of pulses delivered during antegrade passage and retrograde catheter retrieval. A post-lithotripsy angioplasty was performed throughout with use of a 1.5mm balloon across the distal DP and pedal-plantar loop and a 2mm balloon angioplasty of the distal AT and proximal DP. Completion imaging demonstrating restored patency through the distal AT, DP and pedal-plantar loop intervention sites noting enhanced opacification of branch vessels throughout all levels of the foot, without noted residual stenosis, contrast extravasation or dissection. Vascular physical exam findings with restored multiphasic doppler signal at distal AT and DP vessels. Clinically, the patient noted complete resolution of ischemic rest pain symptoms with continued healing of digital ulcers. Surveillance arterial duplex at one-month postoperatively demonstrated patency of the DP with multiphasic waveform and restoration of a great toe pressure (71mmHg) adequate for wound healing in CLTI patient (Fig 2).


Charles Bailey is a board-certified vascular surgeon at Emory Healthcare and an assistant professor of surgery at Emory University School of Medicine. He specializes in limb preservation, peripheral arterial disease and complex vascular care.
Case report 2
Roughly one to three million patients suffer from life limiting claudication in the United States8 and approximately 5-10% of these patients evolve to critical limb ischemia,4,5 increasing their risk for amputation.
Understanding that many lesions below-the-knee are chronic total occlusions comprised of calcium,6,7 we effectively utilized the Shockwave Javelin Forward IVL device to modify the calcific plaque and cross the chronic total occlusion (CTO), thus reducing the risk of dissection, perforation and ultimately amputation.
Patient Presentation

A 79-year-old male with a history of coronary artery disease, diabetes, hyperlipidemia, chronic obstructive pulmonary disease and hypertension presented with a failing to heal left great toe wound. He stated that over the last year his exercise capacity has significantly decreased because of a cramp like pain in both calves to the point he could not walk more than 100 yards without having to stop. This issue peaked approximately three months ago when he stumped his left great toe on the edge of the bed opening a wound. He was seen and treated by podiatry with little success in healing the wound. His left toe brachial index (TBI) was 0.2 with blunted monophasic waveforms — therefore, referred for vascular consultation. Considering the location of the wound and the angiosome related artery1,2,3 our focus for endovascular intervention was the anterior tibial artery (ATA). Abdominal aortography and runoff performed of the left lower extremity showed a widely patent left common iliac, external iliac, common femoral, superficial femoral, deep femoral and popliteal arteries. Below-the-knee (Fig 1 and 2), the AT artery showed a 99% proximal stenosis and occlusion above-the-ankle. The posterior tibial (PT) artery showed an occlusion above-the-ankle. The peroneal artery extended above the ankle providing collaterals flow to the distal PT and the medial and lateral plantar arteries. There was little to no flow to the left great toe for healing.

Procedural Details
Endovascular intervention followed, a 5F 90cm sheath was placed to the level of the left popliteal artery and anticoagulating with heparin achieving and maintaining an activated clotting time >250 seconds. We crossed the proximal AT stenosis with a guidewire and performed percutaneous transluminal angioplasty with a 3x200mm noncompliant balloon (Fig 3) for two minutes, resulting in <20% residual and no flow limiting dissections. We then crossed the distal left AT occlusion with a 0.14, 300 cm length hydrophilic coated guidewire to the left great toe digital artery. A low profile 1x15mm balloon would not pass across the distal AT occlusion and therefore chose to use Shockwave Javelin. We slowly advanced the Forward IVL device to the level of the left digital artery utilizing the entire 120 pulses (Fig 4), modifying the calcium and creating a small lumen. Successful percutaneous transluminal angioplasty (PTA) was performed using a 1x15mm balloon. We then used adjunctive non-compliant balloon angioplasty starting with a 2mm followed by a 2.5mm balloon to effectively dilate the vessel from the left digital artery to the distal AT resulting in less than 20% residual and improved flow to the toe wound (Fig 5). The patient’s left great toe wound successfully healed within a period of two weeks with the aid of podiatry. Utilizing the angiosome concept1,2,3 allowed us to select the vessel which supplied direct in-line flow to the wound and the AT artery, which promoted healing.



George Adams is a board-certified interventional cardiologist at UNC Rex Hospital and a clinical associate professor of medicine at the University of North Carolina at Chapel Hill. He specializes in complex peripheral vascular interventions, amputation prevention, and advanced cardiovascular care. Vanessa Adams is a healthcare professional at UNC Rex Hospital with a focus on providing compassionate, high-quality care.
References
- Taylor GI, Corlett RJ, Ashton MW. The Functional Angiosome: Clinical Implications of the Anatomical Concept. Plastic and Reconstructive Surgery. 2017
- Attinger CE, Evans KK, Bulan E, Blume P, Cooper P. Angiosomoes of the Foot and Ankle and Clinical Implications for Limb Salvage: Reconstruction, Incisions, and Revascularization. Plastic and Reconstructive Surgery. 2006
- Taylor GI, Pan WR. Angiosomes of the Leg: Anatomic Study and Clinical Implications. Plastic and Reconstructive Surgery. 1998.
- Farber A. Chronic Limb Threatening Ischemia. The New England Journal of Medicine. 2018.
- Farber A, Eberhardt RT. The Current State of Critical Limb Ischemia: A Systematic Review. JAMA Surgery. 2016.
- Mcdermott MM. Peripheral Arterial Disease in the Legs. The New England Journal of Medicine. 2026.
- Hamur H, Onk OA, Vuruskari E, et al. Determinants of Chronic Total Occlusion in Patients with Peripheral Arterial Occlusive Disease. Angiology. 2017.
- Criqui M, et al. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association. Circ. Volume 144, Number 9. July 2021.
- Corl JD, Clair D, Mwipatayi P, et al. FORWARD PAD IDE/Feasibility Studies: Primary Endpoint Analysis of a Novel Non-Balloon-Based Peripheral IVL Catheter. JACC: Cardiovascular Interventions. Published online November 4, 2024. doi:10.1016/j.jcin.2024.10.035. Corl J, VIVA Late Breaking Clinical Trial 2024.
Charles Bailey and George Adams are paid consultants of Shockwave Medical. The views expressed are those of the authors and not necessarily those of Shockwave Medical.
Shockwave Javelin Peripheral IVL Catheter Safety Information
In the United States: Rx only.
Indications for Use— The Shockwave Medical IVL System with the Javelin Peripheral IVL Catheter is intended for lithotripsy- enabled modification and crossing of calcified lesions in the peripheral vasculature, including the iliac, femoral, ilio-femoral, popliteal, and infra-popliteal arteries, prior to final treatment.
Not for use in coronary, carotid, or cerebral vasculature. Additionally, not for use in pulmonary vasculature in the U.S. and New Zealand.
Contraindications— Do not use if unable to pass 0.014″ (0.36 mm) guidewire across the treatment site-Not intended for treatment of in-stent restenosis or in coronary, carotid, cerebral or pulmonary arteries.
Warnings— Only to be used by physicians who are familiar with interventional vascular procedures—Physicians must be trained prior to use of the device— Use the generator in accordance with recommended settings as stated in the Operator’s Manual.
Precautions— Avoid applying acoustic pressure pulses while IVL window is not filled with sterile saline—Appropriate anticoagulant therapy should be administered by the physician— Decision regarding use of distal protection should be made based on physician assessment of treatment lesion morphology.
Adverse effects— Possible adverse effects consistent with standard angioplasty include-Access site complications -Allergy to contrast or blood thinner- Arterial bypass surgery—Bleeding complications—Death— Fracture of guidewire or device—Hypertension/Hypotension— Infection/sepsis—Placement of a stent—renal failure— Shock/pulmonary edema—target vessel stenosis or occlusion— Vascular complications. Risks unique to the device and its use— Allergy to catheter material(s)— Device malfunction or failure.
Prior to use, please reference the Instructions for Use for more information on indications, contraindications, warnings, precautions and adverse events. www.shockwavemedical.com/IFU
© Shockwave Medical, Inc. All Rights Reserved. SPL 80483 Rev. A.











